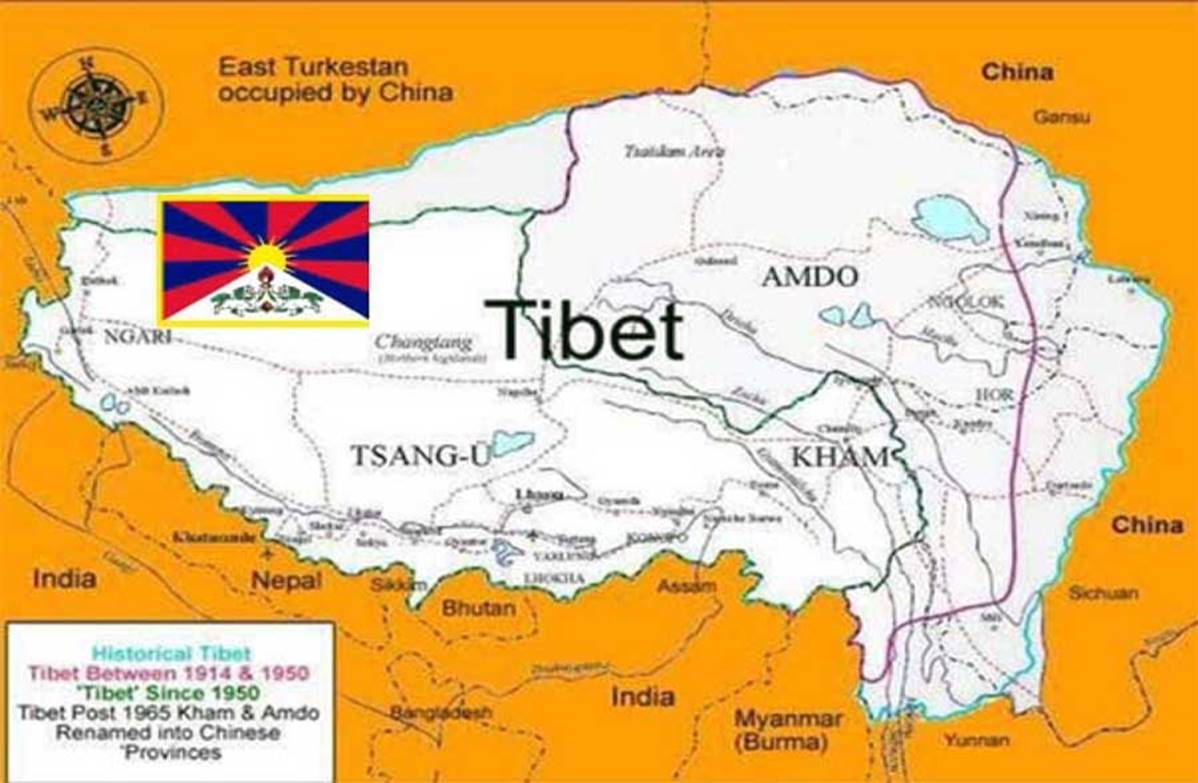
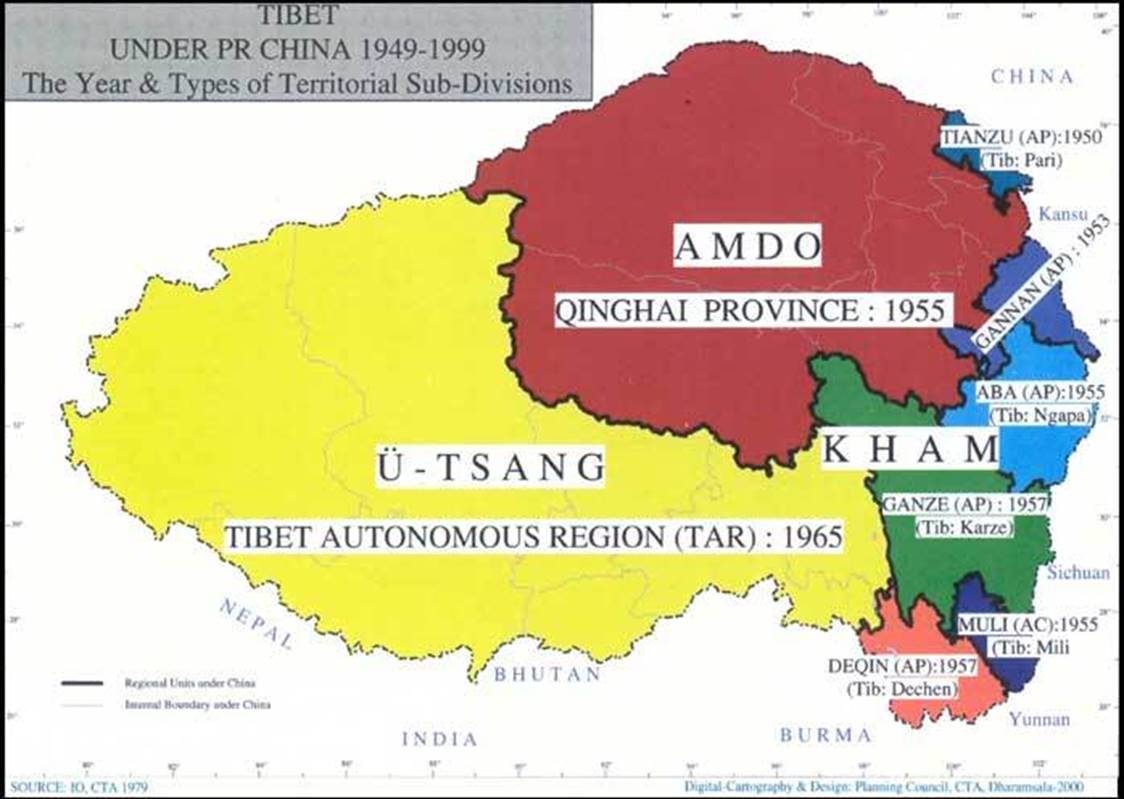
THE TIBET QUESTION – UNITY OF TIBETAN TERRITORY

Living Tibetan Spirits demand Unity of entire Tibetan territory as the first step to resolve problem called ‘The Tibet Question’. During 1974, Special Frontier Force dispatched me to visit Bylakuppe and I spent over four weeks of time speaking to Tibetan children. Tibetans fully understand the boundaries of Tibet and there must be no compromise on this issue.
Rudranarasimham Rebbapragada
SPECIAL FRONTIER FORCE
UNITY OF THREE PROVINCES OF TIBET IS MOST IMPORTANT: HIS HOLINESS THE DALAI LAMA IN BYLAKUPPE
Clipped from: http://tibet.net/2017/12/unity-of-three-provinces-of-tibet-is-most-important-his-holiness-the-dalai-lama-in-bylakuppe/

His Holiness the Dalai Lama addressing recently arrived Tibetan pilgrims from Tibet and Tibetan teachers gathered for a workshop on Secular Ethics in the Sera Lachi Assembly Hall in Bylakuppe, Karnataka, India on 22 December 2017. Photo/Tenzin Phende/DIIR
Bylakuppe: His Holiness the Dalai Lama gave an audience to new arrivals from Tibet and a group of Tibetan teachers gathered for Secular ethics workshop on Friday morning.
“Tibetans in Tibet are the real masters of the country. Despite facing immense hardship, you have kept your spirits up. In 1959, the whole of Tibet was thrown into turmoil. There is a story that after the bombardment of Lhasa, Mao Zedong asked what happened to the Dalai Lama. When he heard that I had escaped to India, he is said to have replied, ‘Then we’ve lost.’”
“The Chinese authorities thought the issue of Tibet would simply fade away, but even after 58 years it hasn’t. In 1959, many countries had no idea about Tibet; they do now,” His Holiness said, urging them to uphold the spirit.
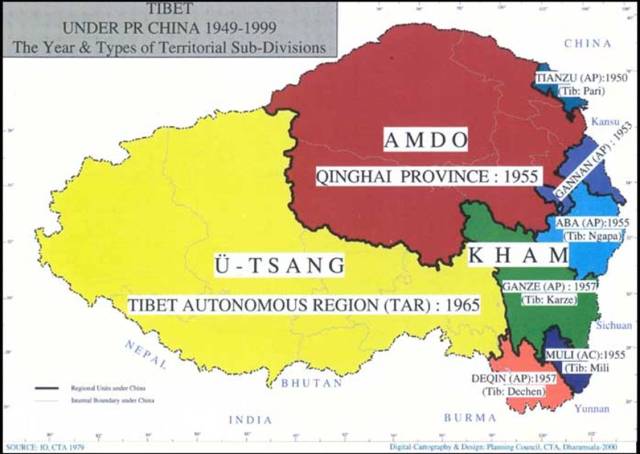
“What is important,” he said, “is that all three provinces of Tibet remain united, standing together in solidarity,” His Holiness told the gathering.
“Tibetans should pride themselves of its thousand millennium old cultural heritage, rooted in the profound Nalanda teachings.”
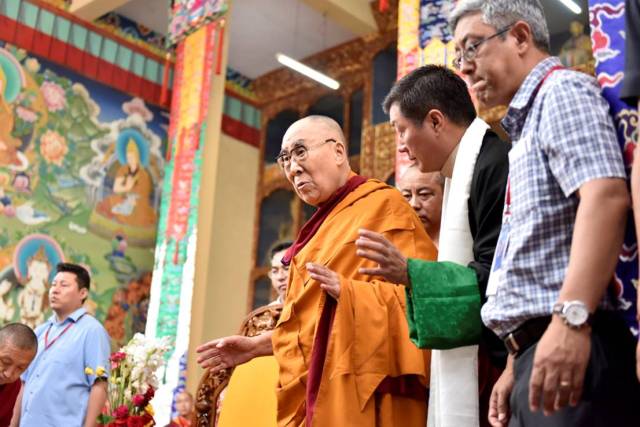
His Holiness the Dalai Lama and President Dr Lobsang Sangay, Central Tibetan Administration arrives at the Sera Lachi Assembly hall to meet the Tibetan pilgrims from Tibet and participants of the workshop on Secular ethics. Photo/Tenzin Phende/DIIR
“We started appealing to the UN late 1959, but, as Pandit Nehru advised me, the USA will not go to war with China over Tibet. We concluded that eventually we would have to deal with the Chinese government. Until now the Chinese policy has been to denigrate the Tibetan people and their culture, nevertheless we remain hopeful of being able to preserve our culture and values within the People’s Republic of China” he added.
His Holiness emphasized “Tibetan language is the key to hold Tibetan alive and unity. Nothing can exterminate Tibetan language which started more than 1000 years ago.”
His Holiness briefly explained about Middle way approach and its appreciation from Chinese intellects.

President of Central Tibetan Administration, Dr Lobsang Sangay addressing recently arrived Tibetan pilgrims from Tibet and Tibetan teachers gathered for a workshop on Secular Ethics in the Sera Lachi Assembly Hall in Bylakuppe, Karnataka, India on 22 December 2017. Photo/Tenzin Phende/DIIR
President Dr Lobsang Sangay, Central Tibetan Administration also addressed the new arrivals and the participants of the workshop on Secular ethics.
In his talk, he emphasized that Middle Way is best approach to have win-win situation and expressed hope for positive changes to take place within China. “The present situation inside Tibet is indeed sad and unfortunate, but I am hopeful that in time, changes will take place within China.”
“We are seeking genuine autonomy for Tibet through non-violence and Chinese government can’t say no to this as it does not contradict China’s sovereignty and One China Policy,” he said.
Enumerating the practicality of Middle Way Approach, under the prevailing situation inside Tibet and exile, Dr Sangay highlighted the widespread support and appreciation expressed by world leaders for the policy envisioned by His Holiness the Dalai Lama.

President of Central Tibetan Administration, Dr Lobsang Sangay addressing recently arrived Tibetan pilgrims from Tibet and Tibetan teachers gathered for a workshop on Secular Ethics in the Sera Lachi Assembly Hall in Bylakuppe, Karnataka, India on 22 December 2017. Photo/Tenzin Phende/DIIR
He further said, “Tibetan in exile practice full democracy rather than Chinese communist party of holding power by few people. Many of high-level authorities are mostly Chinese. So we seek to genuine autonomy, which is within framework of Peoples Republic of China’s constitution.”
President Dr Sangay urged people to invest in education rather than wasting money on luxury. “Since 2011, Kashag has given top priority to education and will continue to do so.”
Towards the end, he urged for the Tibetans to stay united. “Keeping differences aside, if we all work together, the dreams and the aspirations of the Tibetan people in Tibet and in exile will be fulfilled,” the President said.
-Filed by Correspondent Tenzin Phende-

Tibetan teachers gathered for a workshop on Secular Ethics listening to His Holiness the Dalai Lama during their meeting at Sera Lachi Assembly Hall in Bylakuppe, Karnataka, India on December 22, 2017. Photo/Tenzin Phende/DIIR
Created with Microsoft OneNote 2016.






























{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}