


A STORY FROM MILITARY HOSPITAL AMBALA, HARYANA STATE, INDIA :
I served at the Military Hospital, Ambala from July 1970, to September 1971. I served in the rank of Lieutenant during the period of my twelve months Hospital Internship Training. I narrated an earlier experience at the same Military Hospital in my blog post titled ‘Defining Indian Identity-Listen to the Heart’.
I want to recount some of my experiences to understand the nature of human condition and the challenges to human existence. The challenges are many and they are so vastly different. I am choosing to narrate the stories of those individuals whose life was cut short while they had no other health issues that could undermine their ability to live. Padma Sundarji, Lieutenant Colonel D’ Souza, and the athlete at Army Ordnance Corps Centre, Secunderabad fought to defend their existence from the threats of Cancer. I had earlier described the nature of the Immune System that defends the human body from Cancer, infections, and foreign proteins.
This is the story about a very young woman whose life was shortened in tragic circumstances and I want to stress the importance; the medical profession has a duty to avoid costly mistakes while delivering routine care.
When people walk into a government-run clinic or hospital, the usual impression is that a doctor would listen to the complaints in about a few minutes time, make a very quick evaluation, and send the patient away with a prescription.
I had earlier mentioned that in the Armed Forces, the Medical Officers would love to spend time medically examining people who have no apparent sickness as they lay emphasis upon diagnosing a person’s Good Health. I was introduced to aspects of Medical Practice in Army at Military Hospital, Ambala where I learned that writing a prescription should not be our first concern. Major. Mohan Pal Dhir, AMC, the Senior Surgical Specialist of the Hospital at that time of my service, instructed me to converse with my patients and try to know each one as an individual; as a person and not as a diseased entity. In India, we would still follow the cultural norms and do not intrude into personal lives unless the patient desires to discuss all the aspects of their medical history.
During 1971, I was in the Hospital Medical Inspection Room around 8.30 P.M. while my friend Lt. Mohan Lal Dubey, AMC was the Orderly Medical Officer;(Dr. M L Dubey is presently Professor, Department of Parasitology, Postgraduate Institute of Medical Education & Research, Chandigarh, India).
A young woman about 17-years-old accompanied by her father walked into the Clinic. Her father had earlier served in the Indian Army. They were traveling in a bus and she was feeling unwell, and they decided to discontinue their journey. The Military Hospital, Ambala is at a short distance from the Grand Trunk Road and the father knew the Hospital and thought that it would be better to have his daughter checked up before getting back to their village. She could not contribute any further information and did not suffer from any serious illness in her life.
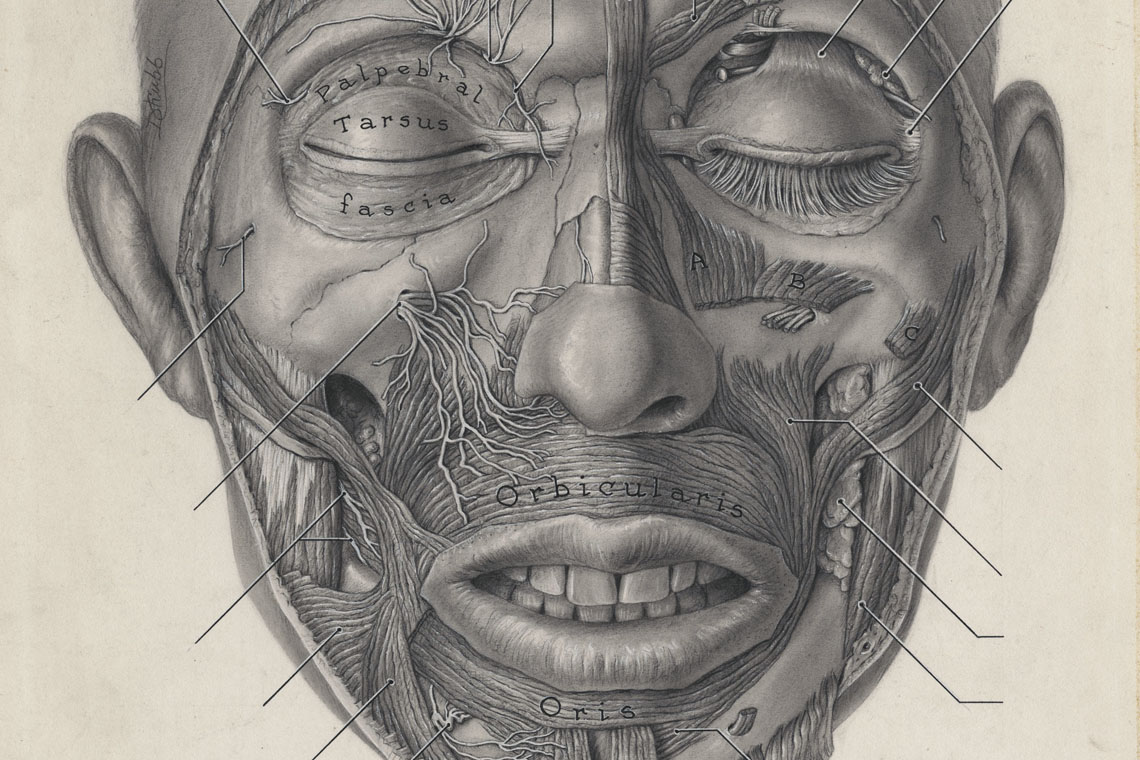
As she walked into the Clinic, I noticed an expression of fear on her face, and it alerted me that there would be some underlying life-threatening problem. Surprisingly, we could not detect any reason( a medical condition ) to explain her feeling of being unwell. Her temperature, pulse, respiration, heart, lungs, and abdomen were all within normal expected limits. I did not want to suggest to this young woman that she was alright. I kept talking to her and her father to arrive at some clues about this sudden sickness that she was experiencing. While speaking to her and intently looking at her face, I noticed with a sense of alarm, that her jaw muscle known as ‘masseters’ appeared to be a lit more ‘taut’.
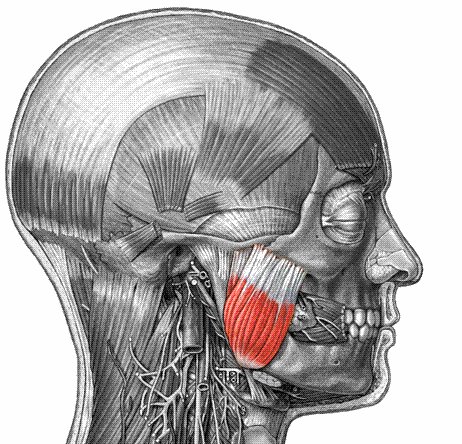
Masseters are the primary chewing muscles. They cover the sides of the jaw just behind the cheeks. These muscles help us to clench our jaws and to grind our teeth. The stiffening of these muscles forced me to think of the possibility of Tetanus infection. Her medical history did not reveal any possibility of contacting this terrifying disease. She had no injuries of any kind.
Myself and my friend Dr. Dubey, checked her again and could not find any evidence of even a minor injury. Her throat, her teeth were normal. She was not hysterical. She was not exposed to drugs or poisons. She had no concerns or experiencing any difficulty about opening her mouth. There was no stiffness of the muscles that she could experience on her own.
This stiffness of jaw muscles, this involvement of facial muscles is the basis for diagnosing the disease of Tetanus. We do not need any laboratory investigations. We need not see the Tetanus bacilli to clinically diagnose this condition. The bacilli live in the intestines of humans, cattle, horses, cats, and dogs without causing any disease. The spores of the Tetanus bacilli are widely distributed in nature, especially in top soil. The spores are very resistant to heat, and chemicals like Lysol and can survive for years in the dust. But, the infection is caused only when the spores enter the body through any wound, particularly like a thorn prick, or a puncture wound caused by a nail, a splinter, or an agricultural implement. The bacilli are strict anaerobes, meaning that they cannot thrive in areas receiving free oxygen. The Tetanus bacilli germinate from its spores only where there is reduced oxygen supply. Generally, a patient would be having a dirty wound or injury. The disease manifests itself very quickly in about 2 days to 2 weeks after the spores germinated in the body tissues. The stiffness of the jaw muscles is called ‘Lock Jaw’ or ‘Trismus’.
We could not conclude that she was a case of Tetanus. The sign of ‘Trismus’ was hanging in the air like a ‘SWORD’. We made a decision to admit her to the Family Ward with the Provisional Diagnosis of ? TRISMUS and initiated the prophylactic treatment against Tetanus as recommended in the Standard Text Books of Surgery. During 1970s, Indian Army Hospitals had no Tetanus Human Immunoglobulin, the antitoxin that is used in the United States to neutralize the neurotoxin produced by tetanus bacilli. We were then using Tetanus Anti-Serum that is procured from horses. This Serum could cause some serious side-effects, and very high doses are not recommended unless treating established Tetanus. She was given an initial dose of 5,000 International Units with due precautions. In India during 1970s, and prior to it, the children were not routinely immunized by ‘triple vaccine’ which is very effective against Tetanus infection. As a precaution, she was also started on Penicillin antibiotic and initiated immunization against tetanus with a dose of Tetanus Toxoid injection. I went away hoping that the stiffness of jaw muscles that I had discovered on my examination would go away and that she would be alright.
Next day, when I arrived at the Hospital at about 7.00 A.M., I came to know that the suspicion of Tetanus became stronger and the patient was transferred to the Intensive Care Room at the Acute Surgical Ward. The Surgeon treated her very vigorously and she survived this terrifying ordeal of Tetanus for five days and lost her battle. She received medical attention as soon as she started experiencing illness, and yet could not be saved.
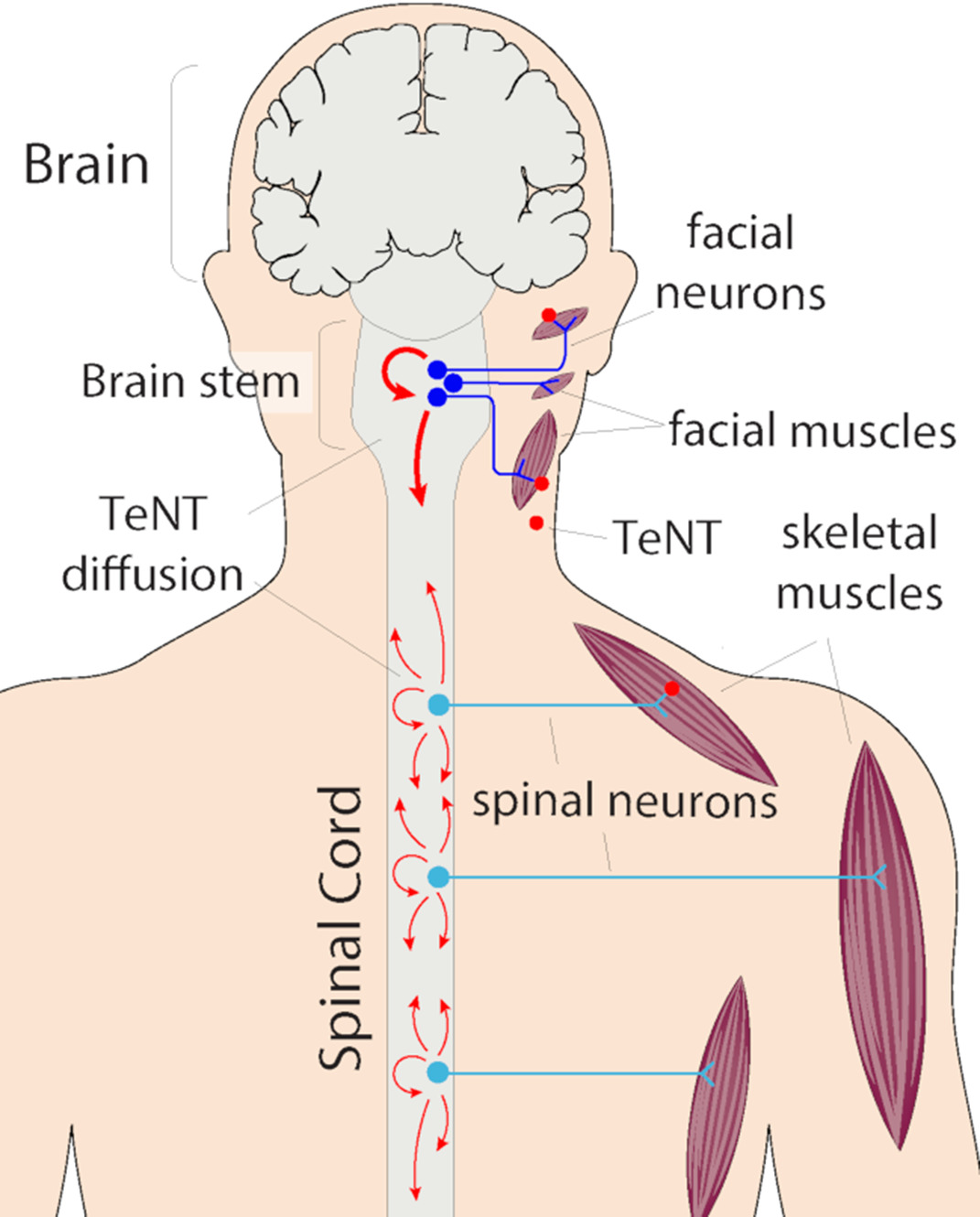
We failed because we could not discover the seat of her infection. The tetanus bacilli after entering human body do not circulate in the blood. They remain stationary at a place where they thrive. The bacilli do not directly harm the body. It is the ‘tetanospasmin’, the neurotoxin that they excrete which circulates in the blood and reaches the neuron cells of the spinal cord that inflicts the damage. It is one of the deadliest poisons known.
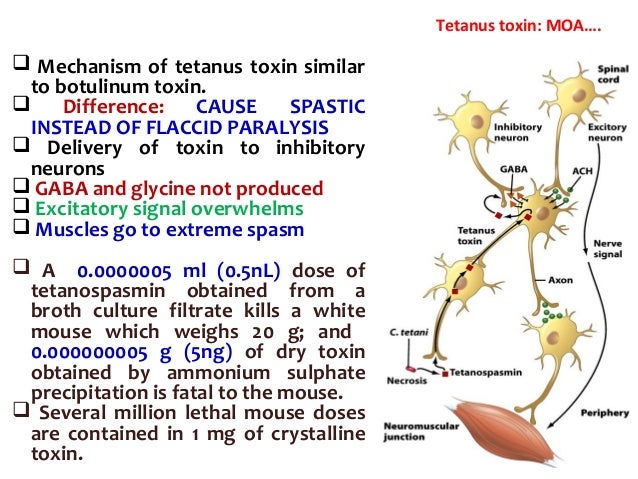
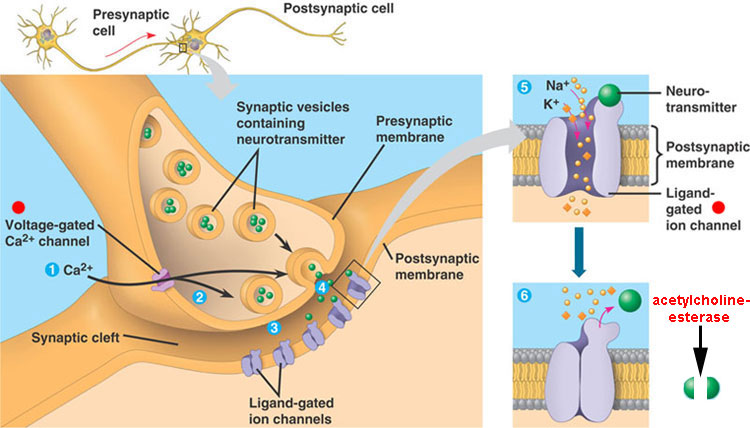
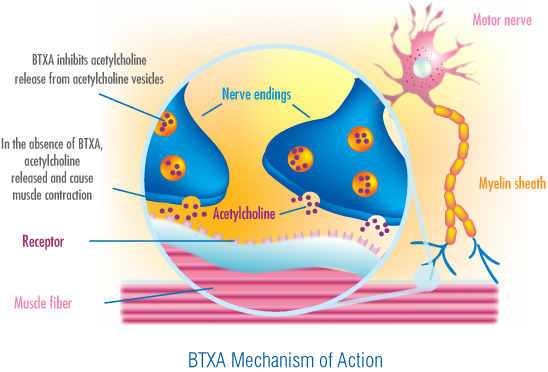
The poison is like the poison known as ‘STRYCHNINE’ which is used to kill rats. The poison specifically acts on the synthesis and release of ‘Acetylcholine’, a chemical that has a key role in the transmission of nerve impulses throughout the body. The stimulation, the accumulation of ‘acetylcholine’ results in rigidity of muscle groups of different voluntary muscles. This toxic rigidity of muscles gradually involves face, head, neck, trunk, extremities and the muscles of respiration. This rigidity of the body is punctuated by sudden tonic spasms, and convulsions. The patient would be exhausted and dies due to respiratory failure. Patients are nursed in dark, very quiet rooms, and are not disturbed and moved without reason. If the seat of infection is known, surgery is performed to completely clean the wound and remove all dead tissue where the Tetanus bacilli multiply.
In this young woman, we could not detect the seat of infection while she was treated. After her death, the Hospital conducted an autopsy to discover the problem. We could conduct this autopsy as her father gave us the necessary permission. Apparently, he understood our anxiety to discover the seat of this infection that took away her precious life.
The Hospital Pathologist, Major B K Sharma, AMC who conducted the autopsy informed me that he isolated the Clostridium.tetani bacilli from the lining of her uterus or womb. Apparently, she acquired a ‘Surgical Infection’ after undergoing a simple gynaecological surgical procedure commonly known as ‘CURETTAGE’ in which the lining membrane of the uterus is gently scraped and removed. The father and the patient did not reveal this information to us.
A sense of Modesty and Cultural Sensitivity could have prevented them from disclosing confidential health information. The operation was done in a Clinic or Hospital and we could not obtain any details. The surgical instrument that was used in this procedure was contaminated with dust carrying the Tetanus spores. The spores cannot be killed by autoclave or sterilizing the instruments at 121 degrees centigrade temperature.
This young woman might have experienced a relatively harmless disorder of her menstrual function which may not truly require a surgical treatment. But, we have no treatment for a disease called ‘GREED’. A medical practitioner sometimes performs a surgical procedure to justify charging a patient a large amount in fees to fill up his/her pockets.
In the autopsy examination, we could not find any reason as to why she was subjected to this Surgical Intervention which introduced this deadly infection into her body. She had no other complications from this surgical operation and she had no gynecological problems and our careful examination did not indicate any problem.
As a rule, doctors do not carry out a gynecological pelvic examination in young patients and particularly when they are not married and have no symptoms and signs of a gynecological disease. Even if we had known, we could not have done more to save her life. She was not evaluated by the Gynaecologist at the Military Hospital, Ambala. I would not think that a Gynecologist would have done the operation of ‘CURETTAGE’ for a second time to get rid of Tetanus bacilli from the endometrial lining of her uterus. It could pose risks of its own. An emergency hysterectomy could be life saving as it would have eliminated the source of neurotoxin production and would have given us a chance to fully neutralize the circulating neurotoxin. Tragically, she got caught up in a situation with no further escape.
BHAJA GOVINDAM:
We exist at the mercy of our LORD. It is not always easy to defend human existence. This tiny bacillus needs no oxygen for its survival. The antibiotics that we may use may not even reach it in enough concentration. The bacillus has a cell wall coated with sugar molecules which may even prevent the antibiotic from entering the cell. A person even with exceptionally strong and well-developed muscles cannot defend himself from this poison. Only timely immunization is the best way to protect a person. During 1970, a spent a month at the Kurnool General Hospital, Kurnool doing my Internship in Medical Ward III. As an Intern at the Medical Ward, I did a neurological examination of a young male patient with well-built body. He was admitted for Spasticity of muscles of his limbs, and the trunk. He was rigid like a board but did not experience any muscle spasms or convulsions. I diagnosed him as a case of Tetanus and transferred him to the Infectious Diseases Ward as per the Hospital Policy. These were the two instances when I made the Clinical Diagnosis of Tetanus and they are important and live in my memory and constantly remind me to seek the protection which only the LORD provides.

Dr. R. Rudra Narasimham,
Kurnool Medical College, Kurnool, A.P., India.,
M.B.B.S., Class of April 1970.


Comment sent by Dr.M.L. Dubey,Professor, Department of Parasitology, Postgraduate Institute of Medical Education & Research, Chandigarh, India :
“I read all the cases described by you and I also noted the reference to my name in account of that case of tetanus in young girl. It took me to nostalgic memory of our days at M.H. Ambala in 1970-71 and our association there.”
LikeLike
I am an Anesthesiologist and now working in Kuala Lumpur. I read this post while preparing for a lecture. I was immediately drawn back to my stay in Ambala until 1969 and had some nostalgic memories of my father The Major S. C Paul who worked as a registrar at the hospital.
i would also like to know the source of your second last picture if you dont mind.
LikeLike
Dear Dr. Dutta,
I am indeed pleased to read your comment. I am glad to hear that you spent time in Ambala. I love that place. Kindly refresh my memory about your father, Major SC Paul. I had arrived at MH Ambala to do my internship (as a Lieutenant) on completion of my training at AMC Centre & Officers Training School, Lucknow(BMOC 20/70) during September, 1970. Major B K Sharma, Pathologist worked as the Registrar of the Hospital. Your father could be the 2 I/C or Second-in-Command, but I am not sure. Would you like to share any photo images of your father? The pictures that I shared in my post were found on Internet and I am not the original source of any of those images. Such use of images is allowed under the Law. Would you like to comment on the case management?
With very best regards,
LikeLike
Dear Dr. Susmita Dutta,
Kindly confirm if your father had served as the Additional Director of Medical Services(ADMS) in the rank of Colonel at First Armoured Division(popularly known as the Black Elephant Division) during 1976 while Major General K S Sundarji was the General Officer Commanding(GOC) of the Division. I had served under Colonel S C Paul while he was our ADMS.
LikeLike
Dear Sir,
Yes indeed, my father was in Ambala in 1976 and ADMS and GOC in C. Was Maj. Gen.. Sundarji.
I have forgotten the name of the battalion.
If so you must have known my father. What a small place the world is.
He died early in 1981 january.
Where do you live now.
Perhaps you could let me know something about my father from your perspective.
With kind regards,
Susmita Dutta
LikeLike
Dear Dr. Susmita Dutta,
Thanks for your kind response. I am sorry to learn that your father passed away in January 1981. It could be a coincidence that your father, and myself got the opportunity to serve in Ambala around the same time. The first time, I had missed him. I had arrived at 55 Medical Battalion during May 1976 from Armed Forces Medical College, Pune. But, after a few weeks, I had to undergo the Medical Officers Junior Command Course(MOJC 67/76) and was away from Ambala from June 07, 1976 to September 03, 1976. After this Course, I had arrived in Ambala with my wife and daughter. We called on your father and met him at his residence and had a chance to meet your mom. We had a very pleasant evening conversing with your parents. But, during that conversation, I do not remember that we may have talked about you. I had to immediately leave Ambala for taking part in a military exercise and your father had asked me to return to Ambala after about a month as I had to participate in a medical conference held at AFMC, Pune during which I had received the DGAFMS Medal. At the First Armoured Division, we had several Family Welfare Clinics and my wife had worked at all those Regimental Clinics as MO and my wife had also met your father when she was first employed by the Armoured Division Units. Were you in Ambala during 1976? I do not remember as to when your father got posted out. It was a very busy tenure due to a variety of training activities and temporary duties at other locations. Unfortunately, I had no opportunity to interact with your father on a regular basis but he had given me his appreciation when I had received the DGAFMS Medal. I have shared two stories about my second tenure in Ambala. If you have time, you may like to review them. I left India during January 1984 and have been living in Ann Arbor, Michigan, USA since 1986 after serving in the Sultanate of Oman for over two and half years. I do not know if you had known the Medical Officers who had served in 55 Medical Battalion during 1976. We had Lt Col Hoare as CO and he got posted to MH Jammu. Our Second-in-Command was Major KS Adhikari who got posted to MH Jullundur.
LikeLike